BANA Offering support and information for people affected by Acoustic Neuroma
BANA (British Acoustic Neuroma Association) has designed this website for people affected by acoustic neuroma (Vestibular Schwannoma) using information gathered from traceable sources. In addition to the public areas of the website, there is also a Members’ only section, accessible right now by all BANA members through their Member’s Login.
A full list of member benefits can be found at Benefits of Becoming a Member
Upcoming events
-
02
May
Come and join our Virtual Support Group Meeting
Virtual Support Group Meeting for Acoustic Neuroma Patients. An online support group for support and information for patients. A welcoming…

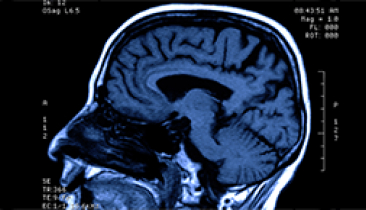
About Acoustic Neuroma
What an acoustic neuroma is, how it is found and the management options
Treatment Options
A full overview of the three management options for acoustic neuroma patients

Related Conditions, Symptoms & Effects
A full overview of the three management options for acoustic neuroma patients
Latest News
-
Greig Frankland-Wilkinson fundraiser for British Acoustic Neuroma Association
So here we go again… a year ago I did the Brighton Marathon so I’m really looking forward to doing…
read more -
Spring into Spring Fundraising Challenge
To support BANA’s ongoing aims we invite you to take part in this fundraising challenge. Beginning on 1st April, start…
read more -
Rochelle’s 30th ANniversary Skydive fundraiser for BANA Fundraising for British Acoustic Neuroma Association CIO
30 years ago on 6th April 1994, I underwent lifesaving & lifechanging surgery to remove a Brain Tumour (Acoustic…
read more
From our gallery









Leading the way in treating acoustic neuroma
For many patients and their families, a tumour diagnosis – like an acoustic neuroma is a stressful time. There are now treatment methods that can be used in case of such a diagnosis.
.